Clinical Pearls
Any good treatment starts with a thorough evaluation, which always includes interview, observation and motion testing, at a minimum. In treating rib dysfunctions, a good deal of valuable information also comes from the palpatory examination.
For example:
a patient who states “my shoulder hurts when I reach into the back seat of the car” during the interview, should raise a flag of concern about an anteriorly-displaced second rib ipsilaterally.
Observing a sub-clavicular fullness can further the hypothesis.
Motion testing the second rib should disclose hypomobility to posterior glide and may provoke characteristic discomfort.
I usually start the physical exam of the ribs by motion testing first ribs, keeping in mind the influence of the lateral cervical muscles as well as the first thoracic vertebra.
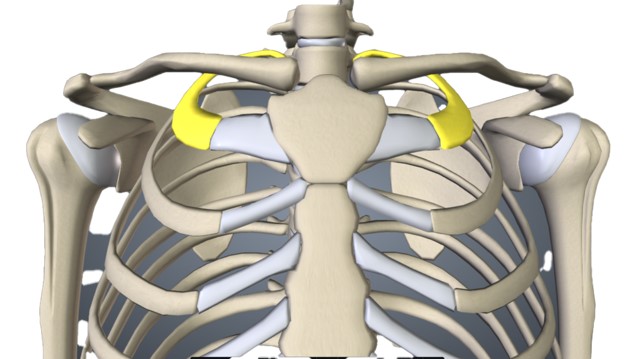
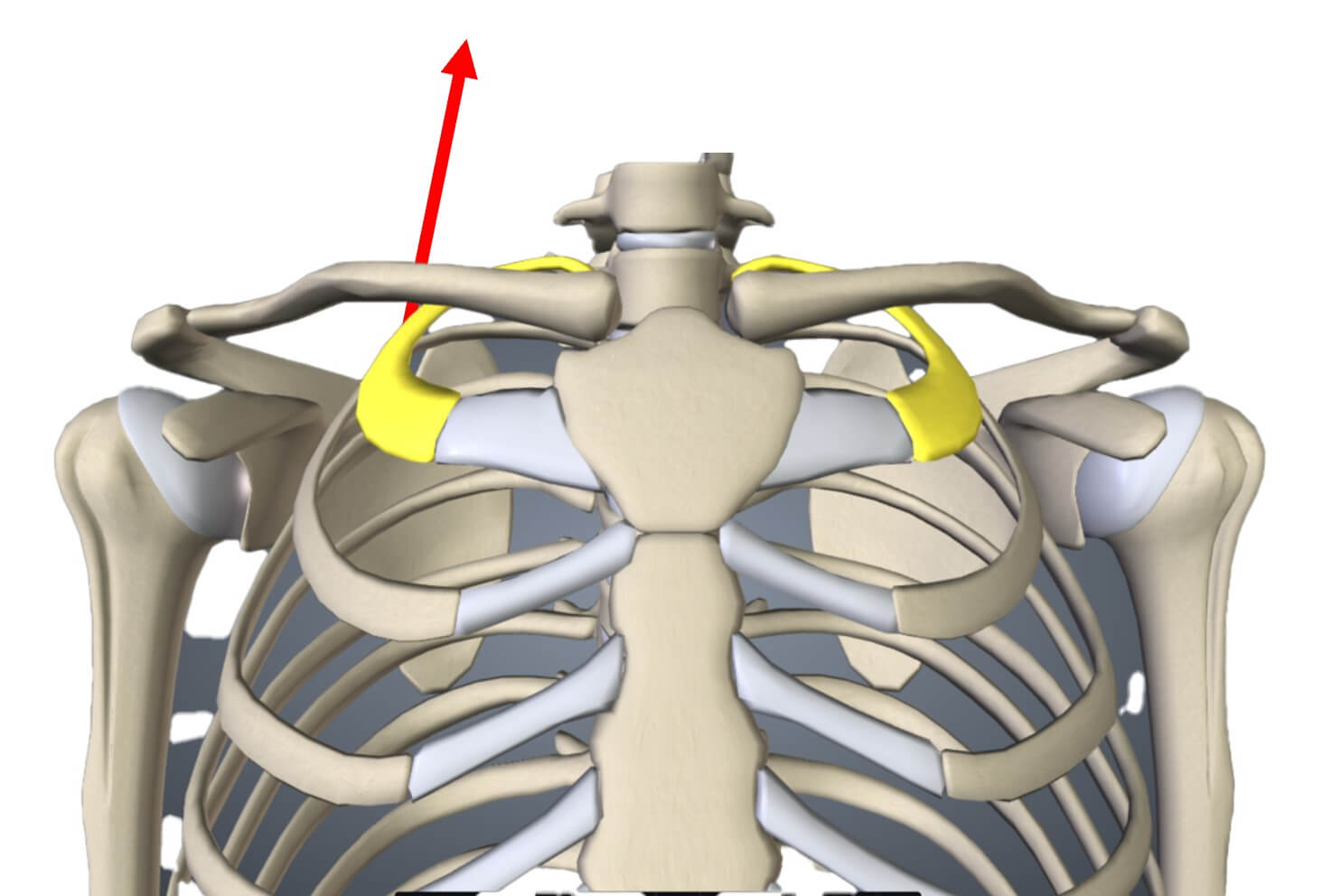
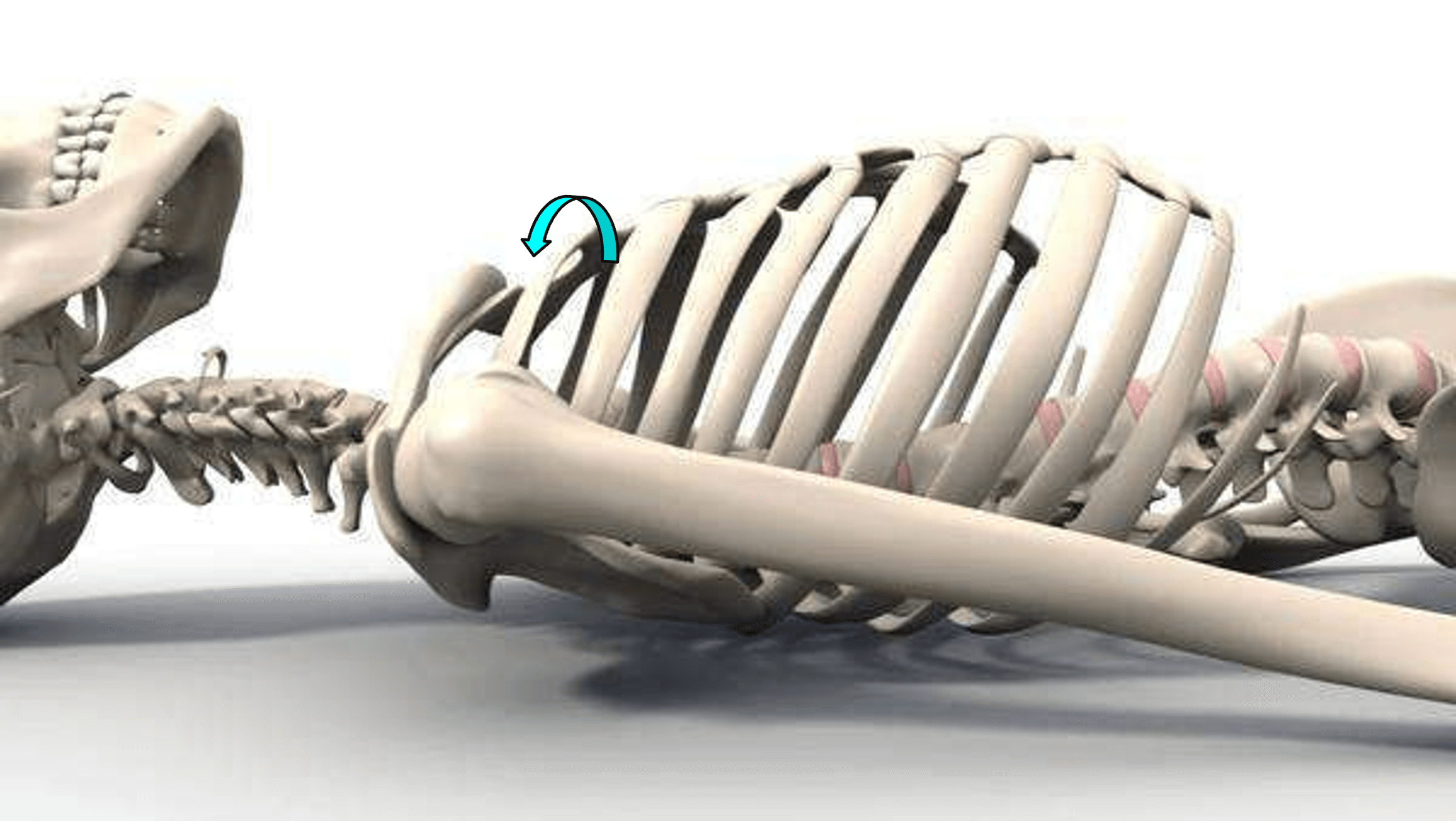
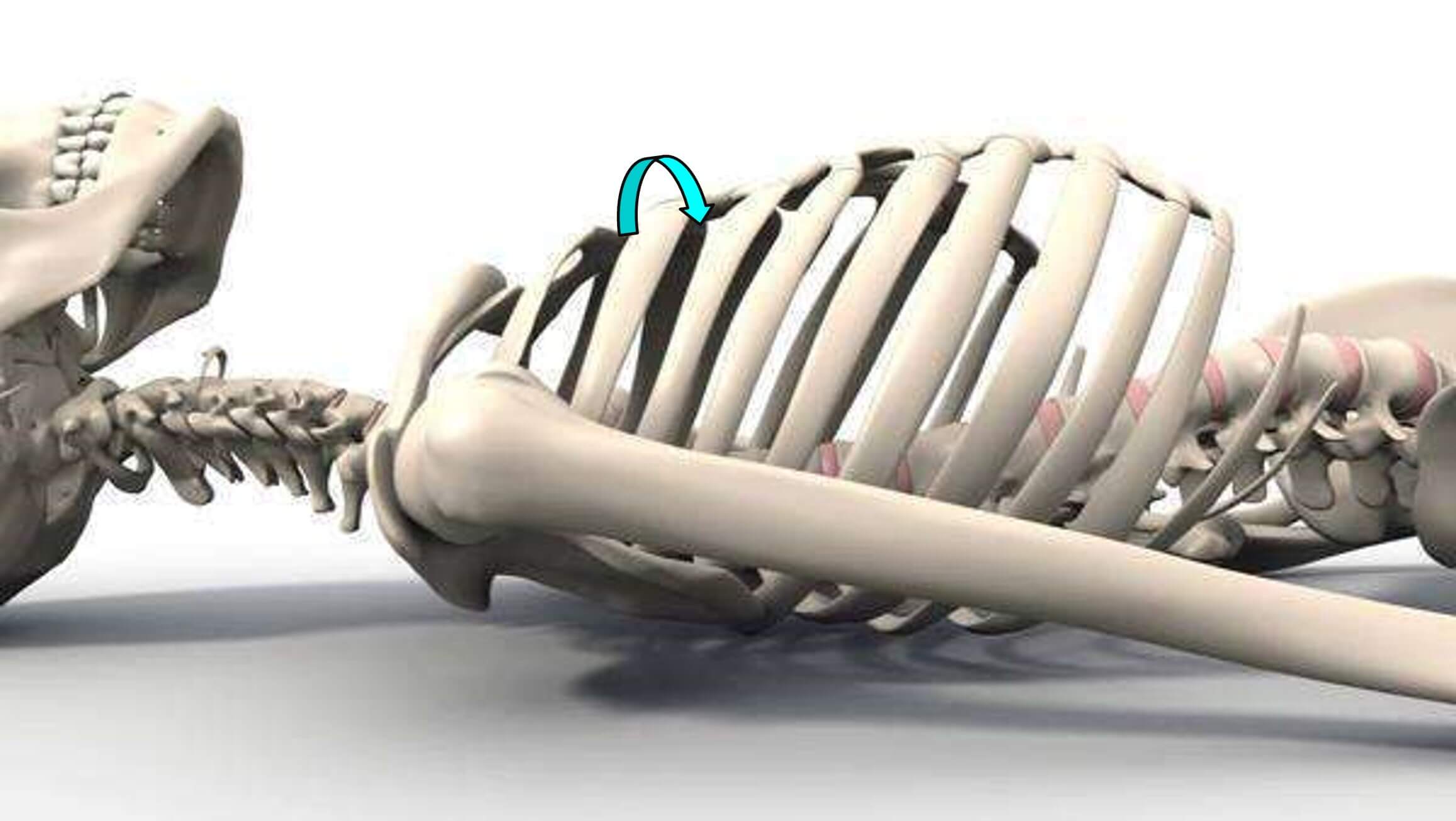
Then checking the clavicles bilaterally for anterior/posterior displacement, inferior/superior displacement and lastly rotation. There are small depressions on the medial end of each clavicle that should line up. A superior/inferior difference between these depressions with no other clavicular asymmetry, suggests a rotational displacement.
The involved clavicle is revealed as hypomobile on motion testing.
Next we can examine the rest of the ribs, keeping in mind that rib lesions can:
♦ occur secondary to vertebral lesions, but the rib lesion can also be primary.
♦ cause intense pain because of their connection with the intercostal nerves.
♦ limit joint motion, at both vertebral and shoulder joints.
Primary rib lesions should be treated effectively as described below.
Rib lesions not easily treated should raise the likelihood of a rib lesion secondary to a primary vertebral lesion.
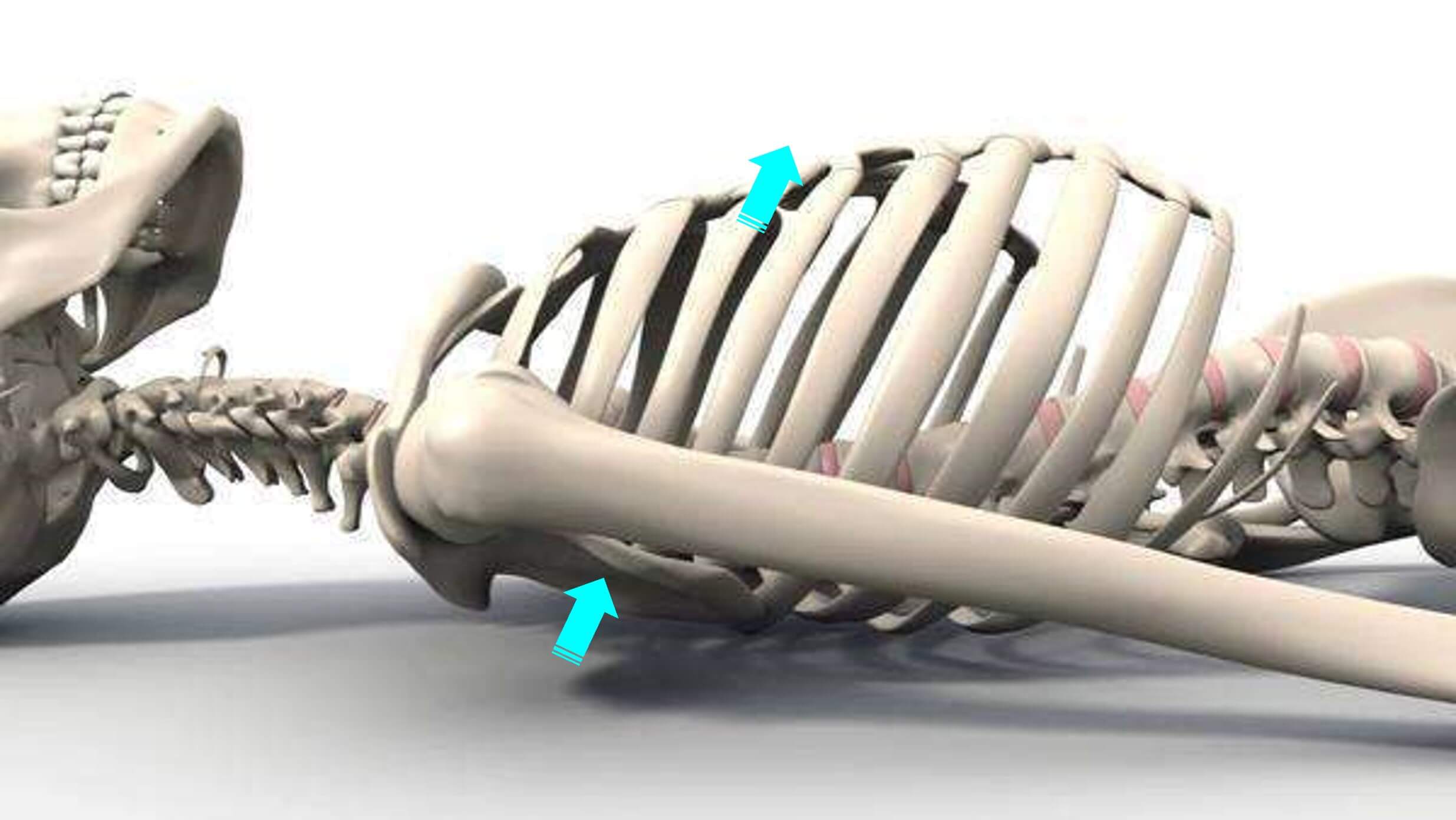
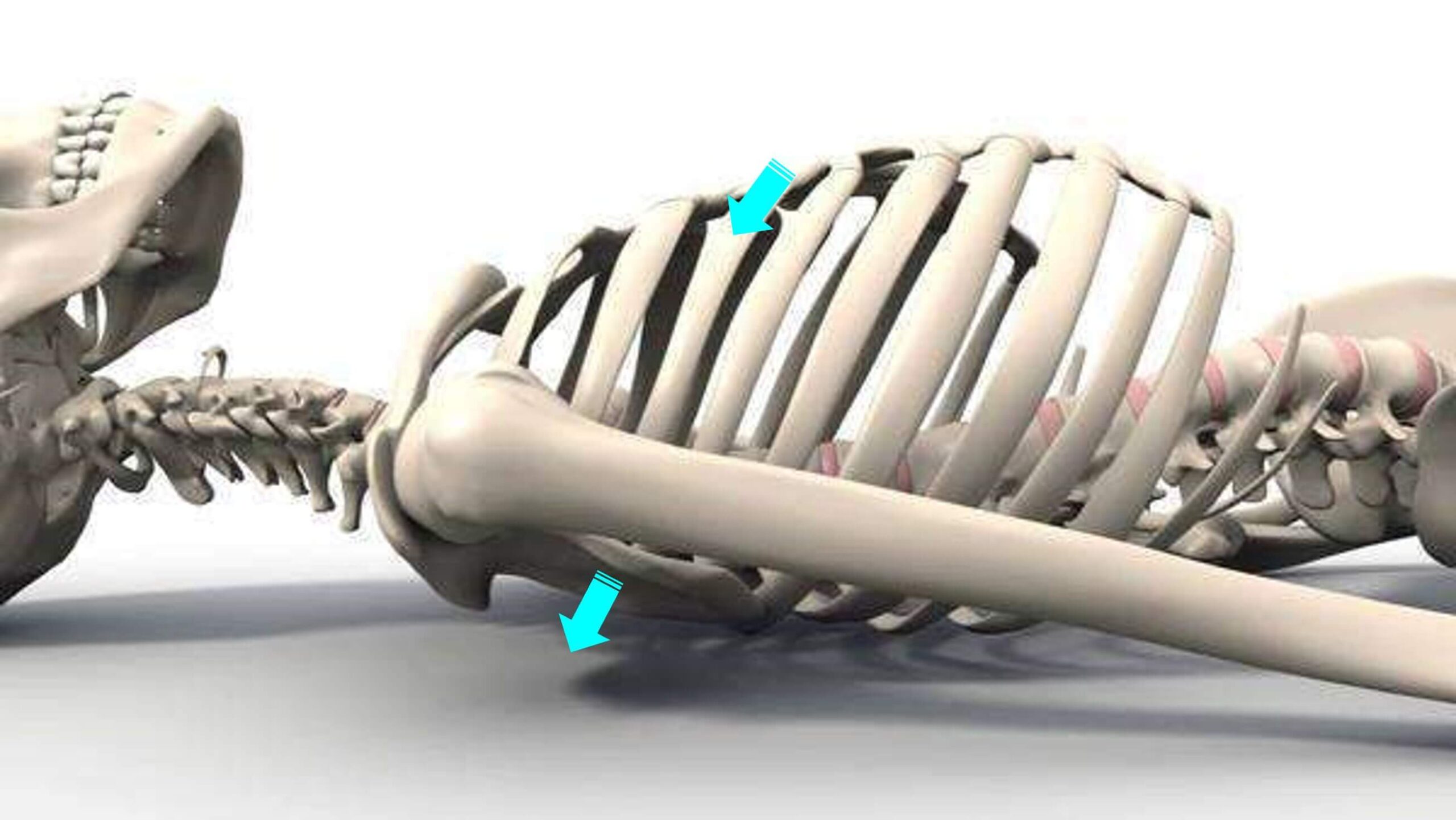
We can find respiratory restrictions due to inhaled (superiorly subluxed) or exhaled (inferiorly subluxed) ribs, but in my experience these are relatively rare, compared to anterior/posterior displacements, medial compressions and torsions.
Contralateral comparisons can be valuable as an initial screen but are fraught with additional confounding variables compared to same-side palpation.
Evaluating ribs in order on the same side makes deviations from what should be a smooth sequential progression more immediately obvious, in my experience.
Any deviation should be identified from the front and from the back to ascertain its nature.
This can be done in almost any position, but a supine patient position makes this task easier for all concerned.